
When faced with a sore throat and difficulty swallowing, the question of the type of tonsillitis is key. Is it simply a temporary irritation or an infection requiring intensive treatment? Tonsillitis is technically defined as an inflammation of the tonsils and the oropharynx. Whilst an infectious cause is the most common, the pain may also stem from excessively dry air, tobacco smoke or overuse of the voice. To treat it properly, it is therefore necessary first to identify the microorganism responsible: a virus or a bacterium.
What are the characteristic symptoms for identifying each type of tonsillitis?
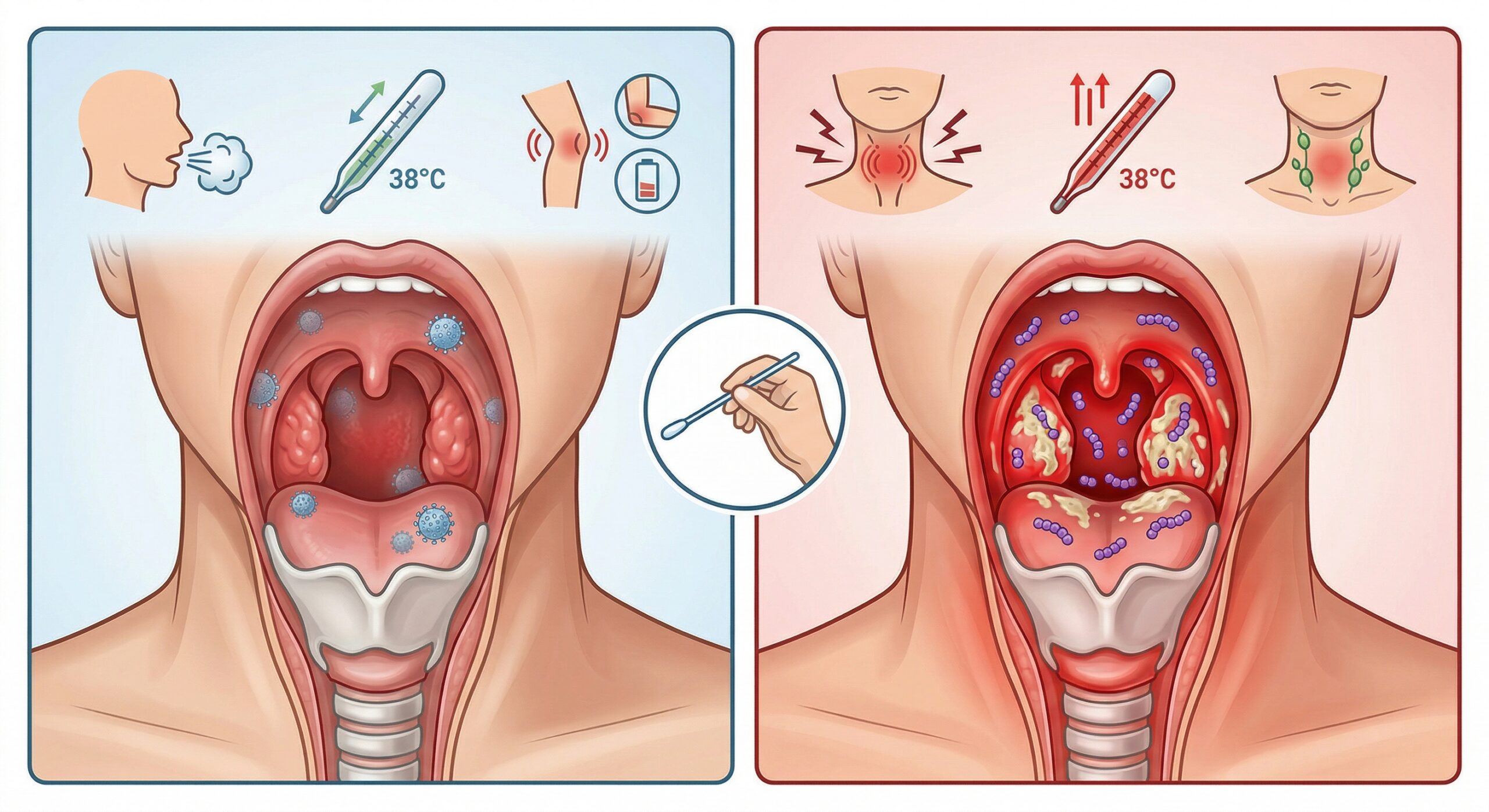
Diagnosis begins with observing the clinical signs, which we have summarised in the following table:
| Characteristics | Bacterial Tonsillitis (Streptococcus) | Viral tonsillitis (50–90% of cases) |
| Epidemiology | Winter and spring. Peak incidence between 5 and 15 years of age. Rare before the age of 3 and after the age of 25. | All year round. |
| Onset of symptoms | Sudden | Gradual |
| General signs | Severe dysphagia (pain), no cough, high fever (> 38°C). | Moderate dysphagia, cough, hoarseness, diarrhoea, joint pain. |
| Local signs | Intense pharyngeal erythema, exudates (white spots), tender neck lymph nodes. | Possible vesicles, associated conjunctivitis. |
| Sore throat test (TDR) | Positive: detection of group A beta-haemolytic streptococcus. | Negative. |
| Treatment | Antibiotics essential Analgesics and antipyretics. | Painkillers and antipyretics only. |
| Progression & Risks | Risk of scarlet fever, acute rheumatic fever or renal complications. | Spontaneous recovery within 3 to 4 days without complications. |
In order to determine the most appropriate treatment, it is necessary to diagnose the type of tonsillitis using specific tests.
How does the rapid diagnostic test confirm the type of streptococcal tonsillitis?
As symptoms can sometimes overlap, modern medicine uses the Rapid Diagnostic Test (RDT), also known as the Streptatest. This test, which can be carried out at a pharmacy or GP surgery, is therefore the most appropriate way to determine the cause of your sore throat. The healthcare professional takes a swab from the tonsils to detect the presence of streptococcus.
The stakes are high: only sore throats caused by Group A streptococcus warrant the prescription of antibiotics. Since the 1999 consensus conference, experts have recommended that only these specific forms be treated with antibiotics. This is particularly important for those under 25, to avoid serious complications such as acute rheumatic fever or glomerulonephritis (kidney damage). To aid decision-making before the test, the Mac Isaac score is used. This score assesses risk based on four criteria: fever, exudates, swollen lymph nodes and absence of a cough.
What are the atypical forms and rarer types of tonsillitis?
Beyond the classic erythematous (red) or erythematopultaceous (white) forms, there are rarer types of tonsillitis whose diagnosis relies on specific laboratory tests.
Among the bacterial causes are Vincent’s angina, an ulcerative form that is often unilateral; syphilitic angina, characterised by an indurated ulceration; and gonococcal angina. More serious still, diphtheritic angina is recognisable by its adherent ‘false membranes’. As for viruses, infectious mononucleosis can also cause pseudomembranes, whilst herpangina manifests as small vesicles. Each variant requires targeted management, as poorly treated tonsillitis can lead to scarlet fever or localised complications.
What are the conventional treatments for relieving each type of sore throat?
Pharmacological management is based on two pillars: pain relief (symptomatic) and, if necessary, eradication of the bacteria (curative).
Managing pain and inflammation
To reduce fever and relieve pain, paracetamol (Doliprane®) remains the preferred standard treatment. In cases of severe inflammation, anti-inflammatory drugs such asibuprofen (Advil®, Spedifen®, Nurofen®) may be used, but please note: they are strictly contraindicated during pregnancy and in people with asthma.
To specifically reduce throat swelling, your pharmacist can recommend local anti-swelling treatments containing alpha-amylase (Maxilase®), available as a syrup or tablets.
Local treatments: sprays, lozenges and antiseptics
Local treatment allows you to act directly on the painful area to soothe or disinfect:
- Mouthwashes and sprays: Solutions such as Hexaspray®, ColluHextril® or Drill® are generally used at a rate of 6 sprays per day.
- Lozenge: These often contain antiseptics or local anaesthetics (Lysopaïne®, Drill®, Strepsils®). For people with diabetes, opt for the “sugar-free” versions (Oropolis®, Drill® sugar-free).
- Natural solutions: Lozenges containing mucilage (Gelovox®) form a protective film to provide long-lasting relief for the mucous membrane.
- ENT disinfection: Bismuth salts (Pholcone®) are sometimes used for their selective cleansing action, but their use is limited to 3 days without medical advice and prohibited for children under 6 years of age.
Safety advice: Avoid lozenges containing a local anaesthetic just before meals to prevent the risk of choking. Furthermore, do not use antiseptics for longer than 5 days to avoid upsetting your oral flora.
Antibiotic treatment: when is it essential?
If the TDR test confirms a bacterial cause (from the age of 5), antibiotic treatment is necessary to eliminate Group A streptococcus.Amoxicillin, prescribed for a 6-day course, is the first-line treatment recommended by the ANSM. In the event of a penicillin allergy, the doctor may prescribe cephalosporins or macrolides. In some cases of severe pain, a short course of corticosteroids may be added.
Pharmacist’s advice: If you are taking antibiotics, it is strongly recommended that you take a course of probiotics to protect your gut flora and prevent the risk of diarrhoea.
In summary, accurately identifying the type of tonsillitis is the key to a quick recovery without complications.
Whilst an allopathic approach is essential for bacterial forms, it is best complemented by a holistic approach to natural care. Many natural remedies, such as homeopathy or herbal medicine, offer effective support to relieve pain and support the body as the infection progresses.
Frequently asked questions about diagnosis and types of sore throat
Can you have a sore throat without a fever?
Yes, some viral sore throats or irritation caused by excessively dry air or tobacco do not always cause a fever. However, a bacterial sore throat is almost always accompanied by a fever.
Is the Streptatest mandatory to get antibiotics?
It is strongly recommended. Antibiotics are ineffective against viruses. The test helps avoid the overuse of unnecessary medication and ensures treatment is targeted only at the correct type of sore throat.
Why is bacterial sore throat more common in children?
The peak incidence of streptococcal infection occurs between the ages of 5 and 15. This is the period when the immune system learns to recognise these pathogens. Conversely, bacterial tonsillitis is virtually non-existent before the age of 3.
What is pseudomembranous tonsillitis?
This is a type of tonsillitis in which whitish membranes form on the tonsils. It may be a sign of mononucleosis (viral) or, more rarely, diphtheria (bacterial).
When should you seek urgent medical attention?
You should seek immediate medical attention if you have a fever lasting longer than 48 hours, difficulty breathing (dyspnoea), severe pain preventing you from eating, or if your lymph nodes become very swollen.



